Yun-Qi Liu1,
Wei-Qun Zhang2 ![]()
For correspondence:- Wei-Qun Zhang Email: iuyunqi15@gmail.com Tel:+865433258523
Received: 13 April 2016 Accepted: 12 November 2016 Published: 22 December 2016
Citation: Liu Y, Zhang W. Role of glabridin in maintaining residual kidney function in dialysis patients. Trop J Pharm Res 2016; 15(12):2739-2743 doi: 10.4314/tjpr.v15i12.29
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To demonstrate the effect of glabridin on peritoneal function and residual renal function (RRF) in peritoneal dialysis (PD) patients.
Methods: Twenty five patients (age range, 24 - 58 years) with a glomerular filtration rate of above 2 mL/min/1.73 m2 and on PD were subjected to glabridin therapy. The patients were treated daily with glabridin (30 mg) for 6 months. The baseline parameters for serum high-sensitivity C-reactive protein (hs-CRP), vascular endothelial growth factor (VEGF), and transforming growth factor β (TGF-β) were compared with those found after 6 months of glabridin treatment. In addition, end-to-initial dialysate concentration of glucose (D4/D0 glucose), dialyzer clearance of urea (K), dialysis time (t), volume of distribution of urea (V), peritoneal transport status as well as dialysate cancer antigen 125 (CA125) were also compared.
Results: The results revealed a significant increase in mean dialysate CA125 after glabridin treatment (25.6 ± 2.7 U/mL) compared with baseline value (19.7 ± 3.2 U/mL). However, serum hs-CRP, VEGF, TGF-β, CTGF, daily ultrafiltration, D4/D0 glucose, Kt/V, and peritoneal transport status remained unaffected. Residual glomerular filtration rate in all the patients decreased. Glabridin treatment also led to a decrease in the decline of peritoneal function, suppression of elevation of profibrotic markers, and increased mesothelial cell mass in PD patients.
Conclusion: Thus, glabridin is a potent candidate for the treatment of residual kidney function in dialysis patients.
Introduction
There is development of alterations in the peritoneal membrane due to long term PD on regular contact with bio-incompatible components of dialysis solution [1]. PD is characterised by peritoneal damage resulting in ultrafiltration (UF) capacity decline, submesothelial fibrosis, extracellular matrix accumulation, and neoangiogenesis [2]. To repair tissues there is a renin–angiotensin–aldosterone system (RAAS) which acts in association with cytokine transforming growth factor β (TGF-β) [3]. For the prevention of peritoneal membrane damage angiotensin converting-enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) are reported to play a vital role [4].
It is reported that mineralocorticoid receptorantagonists improve the prognosis of patients with kidney injury [5]. Some of the drug candidates like irbesartan, spironolactone, and irbesartan plus spironolactone were found to lower peritoneal fibrosis in rats with bacterial peritonitis [6]. Residual renal function (RRF), the measure of dialysis adequacy and creatinine clearance [7] from the kidney accounts for most of the variability in the requirement for dialysis [8]. It is the major determinant of morbidity and mortality in patients on PD [9]. Although ACEIs and ARBs have been shown to slow the decline in RRF [10].
Glycyrrhiza plant, a member of the Leguminosae family has been medicinally used for more than 4,000 years [11]. Glabridin (), isolated from licorice (root and stolon of Glycyrrhiza) has been reported to possess various pharmacological activities like cytotoxic, antimicrobial, anti-fatigue, estrogenic and anti-proliferative activity against human breast cancer cells [12]. It also affects melanogenesis, inflammation, low density lipoprotein oxidation and protection of mitochondrial functions from oxidative stress [13]. In the present study, we devised an experiment to investigate the protective effects of glabridin on peritoneal function and RRF in PD patients.
Methods
Patients
Thirty patients (age range, 24 - 58 years) with glomerular filtration rate (GFR) >2 mL/min/1.73 m2 and who had no history of taking an ACEI or ARB for at least 6 months and had been on PD for at least 5 months were enrolled for glabridin treatment study. All the enrolled patients were free from underlying medical condition that involves treatment with ACEI or ARB, hyperpotassemia, or an active infection or a peritonitis episode within the preceding 3 month. All the related information such as age, sex, body mass index, blood pressure, cause of end-stage renal failure, and time spent on PD was recorded for all the patients. The patients were daily given 30 mg of glabridin for 6 months and were analysed every month in PD clinic. The patients were recommended regular diet containing 1.0 -1.3 g/kg protein daily and limited sodium throughout the follow-up period.
Ethical statement
The present study was approved by the ethical committee of Zhongshan Hospital, Fudan University (no. 2012 93; Shanghai, China) and conducted in accordance with the declaration of Helsinki [14]. A written consent was taken from all the patients to ensure that they are aware of the nature of the study.
Biochemical tests
For biochemical investigation, the blood samples of fasting patients were collected for blood cell count, and serum levels of glucose, blood urea nitrogen, creatinine, sodium, potassium, calcium, phosphorus, total protein, albumin and triglycerides. Total cholesterol, low-density and very-low-density lipoprotein cholesterol were measured by standard enzymatic methods.
Nephelometric method (Dade Behring, Deerfield, IL, USA) was used for high sensitivity C-reactive protein (hs-CRP) measurement. For the measurement of serum vascular endothelial growth factor (VEGF), TGF-β, and connective tissue growth factor (CTGF) blood samples were centrifuged at 12000 cycles per second for 2 min.
For enzyme-linked immunosorbent assay using a commercial kit (Invitrogen, Camarillo, CA, USA) supernatant was stored at -80 °C. The clearance of urea and creatinine from renal and peritoneal urine and dialysate 24 h collections was measured. Serum urea and creatinine were determined simultaneously and residual GFR was defined as the average of the 24 h urinary urea and creatinine clearances. The standard peritoneal equilibration test using dialysate containing 3 % glucose was used for peritoneal function like daily UF and glucose transport. The electrochemiluminescence assay (Elecys CA125 II kit with an Elecsys 2010 immunoassay analyzer: Roche Diagnostics, Mannheim, Germany) was used to measure cancer antigen 125 (CA125) concentrations in the 24h peritoneal effluent collection.
Statistical analysis
The Statistical Package for Social Sciences (version 15.0 for Windows: SPSS, Chicago, IL, USA) was used for statistical analysis. One-way analysis of variance (ANOVA) was used to determine whether there are any statistically significant differences. The results are expressed as mean ± standard deviation (SD). Differences were considered statistically significant at p < 0.05.
Results
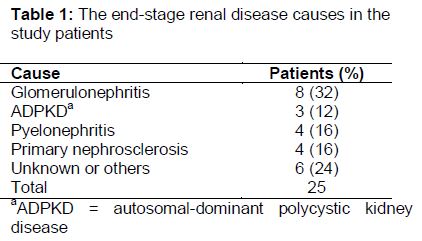
Among 25 patients enrolled for glabridin treatment 16 were male and 9 female with a average age of 49 ± 10 years (range: 24-58 years) and a PD duration of 17 ± 25 months. The causes of end-stage renal disease diagnosed was glomerulonephritis, autosomal-dominant polycystic kidney disease, pyelonephritis and in 6 patients cause could not be detected ().
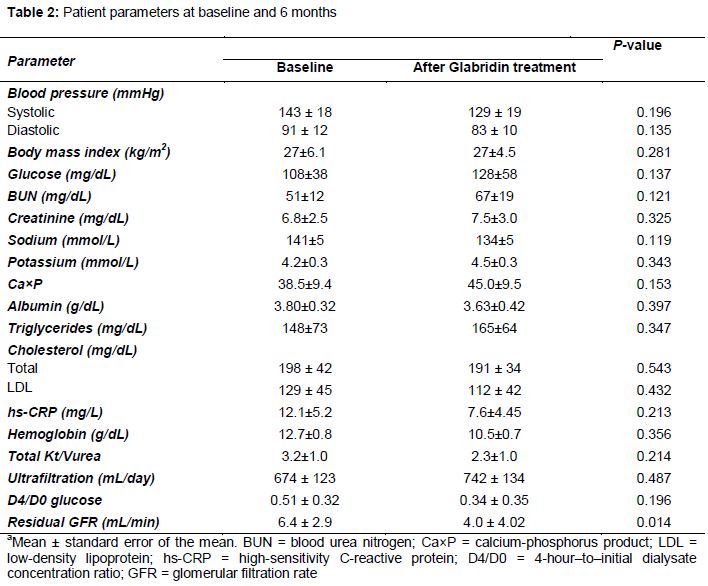
Twenty one patients suffered from continuous ambulatory PD and 4 patients from continuous cycling PD. The examination of various parameters such as glucose, blood urea nitrogen, creatinine, sodium, potassium, calcium, phosphorus, albumin, cholesterol, hs-CRP, and hemoglobin before and after 6 months of glabridin treatment revealed no significant difference (). However, a significant decrease in the peritoneal membrane function decline (UF, D4/D0 glucose, Kt/V urea) was observed at the end of the treatment.
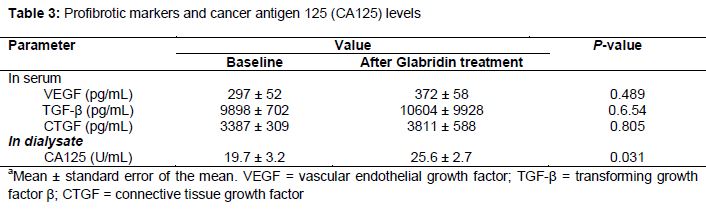
The biochemical examination of the residual glomerular filtration rate (GFR) showed a significant decrease by the end of 6 months of glabridin treatment (3.52 ± 4.31 mL/min) compared with baseline (6.11 ± 4.65 mL/min). Glabridin treatment (25.89 ± 9.78 U/mL) also caused a significant increase in mean dialysate CA125 after 6 months compared with baseline (18.13 ± 9.32 U/mL). On the other hand, glabridin treatment induced no significant change in serum profibrotic markers such as VEGF, TGF-β, and CTGF ().
Discussion
There is development of alterations in the peritoneal membrane due to long term PD on regular contact with bio-incompatible components of dialysis solution [1]. A reduction in peritoneal thickness and enhancement of UF volume by ACEI whereas preservation of RRF and enhancement of peritoneal creatinine clearance by ARB after one year of PD initiation was reported [4,11]. The present study demonstrates the effect of glabridin on peritoneal function and RRF in patients on PD. Glabridin treatment for 6 months did not induce any significant difference in profibrotic markers or in parameters of peritoneal membrane function (UF, Kt/V, D4/D0 glucose). However the dialysate levels of CA125, a useful marker of mesothelial cell mass were significantly increased on glabridin treatment after 6 months. It has been shown that treatment of mesothelial cell culture to high concentrations of glucose caused increase in RAAS activation and angiotensinogen II led to an enhancement of TGF-β. TGF-β plays a vital role as the mediator in the development of fibrosis [3].
Our results revealed no significant difference in the levels of serum profibrotic markers (VEGF, TGF-β, CTGF) after 6 months of glabridin treatment. The levels of these profibrotic markers are expected to increase during the 6 month period after PD initiation in untreated patients. Among various alterations in the peritoneal membrane induced due to long term PD, loss of mesothelial cells is one such alteration. Loss of mesothelial cells is indicated by the dialysate CA125 with respect to the effect of the cell mass on mesothelium [15]. Local CA125 is released by peritoneal mesothelial cells within the peritoneum [16] and studies have shown a relation between the number of mesothelial cells in peritoneal effluent from PD patients and effluent CA125 concentration. In patients with peritoneal sclerosis low CA125 values have been observed. Glabridin treatment caused a significant enhancement in effluent CA125 after 6 months of the treatment. Thus, glabridin treatment leads to an increase in mesothelial cell mass.
Conclusion
The findings of this study indicate that glabridin treatment induces a decrease in the loss of peritoneal function, suppresses the expected elevation in profibrotic markers, and increases mesothelial cell mass in PD patients. Therefore, glabridin is a potent candidate for the treatment of residual kidney function in dialysis patients.
Declarations
Acknowledgement
References
Archives


News Updates